We at Crack4sure are committed to giving students who are preparing for the AAPC CPC Exam the most current and reliable questions . To help people study, we've made some of our Certified Professional Coder (CPC) Exam exam materials available for free to everyone. You can take the Free CPC Practice Test as many times as you want. The answers to the practice questions are given, and each answer is explained.
Refer to the supplemental information when answering this question:
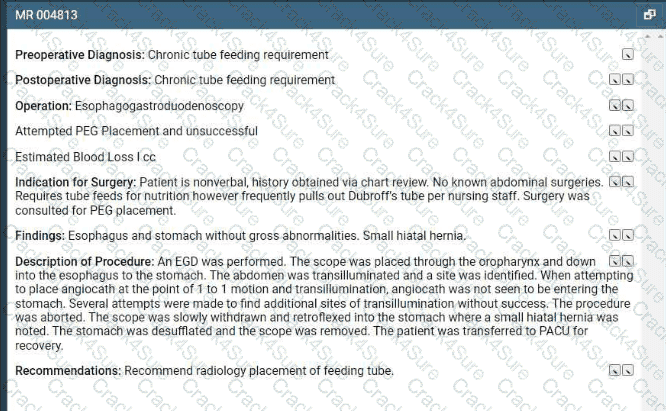
View MR 004813
What CPT® and ICD-10-CM codes are reported?
(Full Case:Pre/Post-op diagnosis:Grade 1 endometrial cancer.Procedure:Radical hysterectomy and pelvic lymph node sampling.Anesthesia:General.EBL:400 mL.Complications:None.Specimens:pelvic washings; uterus; tubes; ovaries; pelvic lymph nodes.Fluids:2 L crystalloid.Operative details:frog-leg position; perineum prepped sterile; Foley placed; midline vertical incision umbilicus to symphysis; exploration shows normal upper abdomen and bowel; no paraaortic adenopathy; pelvis/perineum normal; washings collected; round ligaments transected; retroperitoneal spaces opened; ureters visualized; ovarian vessels isolated/ligated; bladder flap taken down; uterine arteries, uterosacral and cardinal ligaments clamped/ligated; uterus removed; vagina closed; lymph node sampling left then right with removal of lymphatic tissue from external/internal iliac bifurcation to circumflex iliac vein and down to obturator nerve; tumor ~40% endometrial surface with < 50% myometrial invasion; closure in layers; patient tolerated well.Question:What CPT® codes are reported?)
Dr. Meredith sees Mr. Hollis (new patient) for the first time In the Community Rest Home. She documents a visit with medical decision making of moderate complexity. She spends 20 minutes of additional time discussing physical therapy and going over medications. Dr. Meredith spends a total of 90 minutes on that patient that day.
What CPT® coding does Dr. Meredith report?
A patient with abnormal growth had a suppression study that included five glucose tests and five human growth hormone tests.
What CPT@ coding is reported?
A 42-year-old male is diagnosed with a left renal mass. Patient is placed under general anesthesia and in prone position. A periumbilical incision is made and a trocar inserted. A laparoscope is inserted and advanced to the operative site. The left kidney is removed, along with part of the left ureter. What CPT® code is reported for this procedure?
(The physician performs adiagnostic ERCPof the common bile duct with insertion of astentinto the biliary duct. What CPT® coding is reported?)
A patient has suspicious lesions on his feet. Biopsies confirm squamous cell carcinoma. The patient elects to destroy a 0.6 cm lesion on the right dorsal foot and a 2.0 cm lesion on the left dorsal foot using cryosurgery.
What CPT® coding is reported?
View MR 004397
MR 004397
Operative Report
Preoperative Diagnosis: Calculi of the gallbladder
Postoperative Diagnosis: Calculi of the gallbladder, chronic cholecystitis
Procedure: Cholecystectomy
Indications: The patient is a 50-year-old woman who has a history of RUQ pain, which ultrasound revealed to be multiple gallstones. She presents for removal of her gallbladder.
Procedure: The patient was brought to the OR and prepped and draped in a normal sterile fashion. After adequate general endotracheal anesthesia was obtained, a trocar was placed and C02 was insufflated into the abdomen until an adequate pneumoperitoneum was achieved. A laparoscope was placed at the umbilicus and the gallbladder and liver bed were visualized. The gallbladder was enlarged and thickened, and there was evidence of chronic inflammatory changes. Two additional ports were placed and graspers were used to free the gallbladder from the liver bed with a combination of sharp dissection and electrocautery. Cystic artery and duct are clipped. Dye is injected in the gallbladder. Cholangiography revealed no intraluminal defect or obstruction. Gallbladder is dissected from the liver bed. The scope and trocars are removed.
What CPT® coding is reported for this case?
A patient is diagnosed with diabetic polyneuropathy.
Using ICD-10-CM coding guidelines, what ICD-10-CM coding is reported?
A patient presents to the ER with a large sacral pressure ulcer measuring 7 cm. The provider excised the ulcer with 3 mm margins, removed muscle and segmental bone, and performed a layered skin flap closure.
What CPT® and ICD-10-CM coding is reported?
A patient is going to have placement of a myringotomy tube. This tube is placed in the ______ to drain excess fluid.
A patient presents with fever, cough, SOB, and fatigue. PCR test is positive for COVID-19. Final diagnosis: pneumonia due to COVID-19. What ICD-10-CM coding is reported?
The documentation states:
He was then sterilely prepped and draped along the flank and abdomen in the usual sterile fashion. I first made a skin incision off the tip of the twelfth rib, extending medially along the banger’s lines of the skin. This was approximately 3.5 cm in length. Once this incision was carried sharply, electrocautery was used to gain access through the external oblique, internal oblique, and transverse abdominis musculature and fascia.
What surgical approach was used for this procedure?
(A patient with age-related osteoporosis is hospitalized after a slip and fall resulting in fractures to both hips. The physician ordersthree-view imaging of both hips and the pelvis, interpreted by the hospital radiologist. Later the same day, the patient falls from bed and the doctor ordersthree additional viewsof both hips and pelvis, interpreted by thesame radiologist. What CPT® coding is reported?)
Patient presents with flank pain and dysuria and is diagnosed with hydronephrosis. Further testing detects ureteropelvic junction obstruction. The final diagnosis is hydronephrosis due to acquired occlusion of ureteropelvic junction with infection. What ICD-10-CM coding is reported?
A 23-year-old receives MMR and Hepatitis B vaccines without counseling.
What CPT® codes are reported?
A Medicare patient is scheduled for a screening colonoscopy.
What code is reported for Medicare?
(Patient presents to the office for the removal of15 actinic keratoseslesions. The provider destroys these lesions withlaser surgery. What CPT® coding is reported for this visit?)
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required ? limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® coding is reported?
Which place of service code is submitted on the claim for a service that is performed in an outpatient surgical floor?
A pediatric patient with a congenital double inlet ventricle undergoes corrective cardiac surgery. The surgeon performs a modified Fontan procedure to redirect systemic venous blood flow directly to the pulmonary arteries as part of staged repair for a single-ventricle physiology.
What CPT® and ICD-10-CM® codes are reported?
A 56-year-old female patient with a history of degenerative disc disease at levels T2-T3 and T4-T5 underwent a surgical repair procedure. Two surgeons will be working together as primary surgeons
Surgeon X: Carried out the anterior exposure of the spine and mobilized the great vessels, assisted Dr. Z. and performed the closure.
Surgeon Z: Performed a minimal anterior discectomy and fusion at T2-T3 and T4-T5 levels using an anterior interbody technique and solely performed utilizing a structural allograft.
What is the CPT® coding for the two surgeons?
A patient suffers a ruptured infrarenal abdominal aortic aneurysm requiring emergent endovascular repair. An aorto-aortic tube endograft is positioned in the aorta and a balloon dilation is performed at the proximal and distal seal zones of the endograft. The balloon angioplasty is performed for endoleak treatment.
What CPT® code does the vascular surgeon use to report the procedure?
A patient undergoes a laparoscopic appendectomy for chronic appendicitis.
What CPT® and diagnosis codes are reported?
An 8-year-old undergoes tonsillectomy with adenoidectomy for chronic tonsillitis and adenoiditis with hypertrophy.
What CPT® and ICD-10-CM codes are reported?
A 3-day-old died in her sleep. The pediatrician determined this was the result of crib death syndrome. The parents give permission to refer the newborn for a necropsy. The pathologist receives the newborn with her brain and performs a gross and microscopic examination. The physician issues the findings and reports they are consistent with a normal female newborn.
What CPT® code is reported?
A surgeon performed Mohs micrographic surgery on a lesion on the right arm. This required one stage with six tissue blocks.
What CPT@ codes are reported for the Mohs surgery?
A 16-year-old female just moved to the area and is living in a campground with her parents. She has several medical conditions and the parents are unable to take her to a physician ' s office. A physician sees the patient in the campground and documents a medical decision making of moderate complexity. After the visit, the physician spends an additional 25 minutes in a prolonged discussion with the patient ' s parents; he reviews complex and detailed medical records from her previous physicians and completes a comprehensive treatment plan. A care plan with the local hearth agency and a dietician is initiated.
What E/M coding is reported for this visit?
A healthy 35-year-old undergoes EP study and ablation under general anesthesia.
What anesthesia coding is correct?
Regarding the CPT® Surgery Guidelines for a surgical code designated as a " Separate Procedure " , which statement is FALSE?
A woman with vulvar intraepithelial neoplasia (VIN II) undergoes a partial vulvectomy ( < 80%) with removal of skin and deep subcutaneous tissue.
What CPT® and ICD-10-CM codes are reported?
The knee joint consists of which three compartments?
The human shoulder is made of which three bones?
An anesthesiologist medically directs two cases during EGD and colonoscopy in a PS III patient with severe bleeding risk.
What CPT® codes are reported?
A 45-year-old patient comes In with chronic sinusitis that has not responded to medication. The physician decides to use a sinus stent implant to help alleviate the patients symptoms.
The physician inserts the implant into the ethmoid sinus using a delivery system. This implant is designed to keep the surgical opening clear, prop open the sinus, and gradually release a corticosteroid with anti-inflammatory properties directly to the sinus lining. The implant is not permanent and will dissolve over time.
What HCPCS Level II code is reported?
Mr. Woolridge has had a suspicious lesion on his left shoulder for approximately eight weeks that is not healing. On the dermatologist ' s exam of left shoulder blade, there is excoriation and scabbing and the lesion not healing. Patient agrees and wishes to proceed with a punch biopsy of the lesion. A punch biopsy is taken of the lesion and sent to pathology. A simple repair is performed at the biopsy site.
What CPT® and ICD-10-CM codes are reported?
(A driver crashes into a guardrail and sustains a fracture of the anterior fossa cranial base with involvement of thesphenoid sinus, withno CSF leak. The patient undergoessurgical nasal sinus endoscopy with sphenoidotomyto evaluate and treat the sinus injury. No CSF leak repair is performed. What is the correct procedure and diagnosis coding combination to report this service?)
Patient is admitted in observation care on 12/2/20XX in the morning for acute asthma exacerbation. The ED physician requires the patient to stay overnight. Next day, 12/3/20XX the patient is
discharged from observation care in the afternoon. Patient ' s total stay in observation was 16 hours.
What E/M categories and code ranges are appropriate to report?
(A patient presents with dysuria and lower abdominal pain. The physician suspects UTI. Anautomated urinalysis without microscopyis done in the office and isnegative. UTI is ruled out for the final diagnosis. What CPT® and ICD-10-CM codes are reported?)
An abdominal X-ray includes decubitus, supine, and erect views.
What CPT® code is reported?
A 44-year-old female patient came in for a planned laparoscopic total abdominal hysterectomy for endometriosis of the uterus. The surgeon attached the trocars, a scope is inserted examining
the uterus, abdominal wall, bilateral ovaries, and fallopian tubes. The surgeon decided to convert the laparoscopic procedure to an open total hysterectomy because of the extensive amount of
adhesions that need to be removed. A total hysterectomy was performed and due to removal of the extensive adhesions the surgery took longer than normal of 2 hours.
What CPT® and diagnosis codes are reported?
A 58-year-old male suffered an acute STEMI of the inferolateral wall while running a marathon on June 15 and had received treatment. Three weeks later, the patient presents to the ED complaining of SOB and left arm pain. An EKG is performed as well as blood tests. Patient is admitted for further evaluation.
What diagnosis code is reported for this encounter?
(What modifier is appended to indicate that during thepostoperative period, a procedure is performed that wasplanned,more extensivethan the original procedure, or done fortherapeutic reasons?)
A physician orders an obstetric panel that includes syphilis screening using the non-treponemal antibody approach, an automated CBC with manual differential WBC count, HBsAg, rubella antibody, a serum antibody screen, and ABO and Rh blood typing.
What CPT® coding is reported?
Which one of the following terms refers to inflammation of the liver?
A patient presents with fever, cough, SOB, and a recent history of COVID-19. A PCR test was positive for COVID-19. The provider documents a final diagnosis of “pneumonia with history of COVID-19.”
What ICD-10-CM coding is reported?
This 27-year-old male has morbid obesity with a BMI of 45 due to a high calorie diet. He has decided to have an open Roux-en-Y gastric bypass. The patient is brought to the operating room and placed in supine position. A midline abdominal incision is made. The stomach is mobilized, and the proximal stomach is divided and stapled creating a small proximal pouch in continuity with the esophagus. A short limb of the proximal bowel of 155 cm is divided. It is brought up and anastomosed to the gastric pouch. The other end of the divided bowel is connected back into the distal small bowel to the short limb ' s gastric anastomosis to restore intestinal continuity. The abdominal incision is closed.
What are the procedure and diagnosis codes for this encounter?
A 1-year-old patient has bilateral supernumerary digits:
Left digit contains bone and joint ? amputated
Right digit is a soft-tissue nubbin ? simple excision
What CPT® coding is reported?
(A provider documents “pericarditis with effusion” in the assessment. Based on medical terminology, which structure is inflamed?)
(A pathologist performs an analysis usingfluorescent microscopyto evaluate a specimen for inherited or acquiredchromosomal abnormalities. No specific CPT® code accurately describes this service. Which unlisted CPT® code is reported?)
(A patient is diagnosed with agangrenous ulceron theright thighwith thefat layer exposedand is currently being treated. What ICD-10-CM coding is reported?)
56-year-old female is postmenopausal with abnormal vaginal bleeding. Ob-gyn provider performs a hysteroscopy to examine the uterine cavity.
What CPT® code is reported?
(Miranda is in her provider’s office for follow up of her diabetes. Her blood sugars remain at goal with continuing her prescribed medications. When referring to the MDM Table for number and complexity of problems addressed, what type of problem is this considered?)
Which medical term refers to inflammation of the cornea?
A cardiologist uses the hospital ' s equipment for a cardiac stress test as he doesn ' t own equipment for the test. He supervises the test and provides the interpretation and report of the test.
What CPT® codes are reported?
What CPT® coding is reported for a subtotal thyroidectomy for malignancy with radical neck dissection?
A 63-year-old is seen by his. primary care physician for an annual exam. His last exam with the primary care physician was four years ago. He has no complaints.
What CPT code is reported?
A physician sees a patient for the first observation visit, spends 85 minutes, with moderate MDM.
What CPT® code is reported?
911 is called by the physician for an ambulance with non-emergency basic life support to pick up a patient from his office that had fainted. The patient was taken to the hospital. What HCPCS
Level II coding is reported for the ambulance ' s service?
An otolaryngologist performs a tympanoplasty with mastoidectomy, reconstruction of the posterior ear canal wall, and ossicular chain reconstruction.
What CPT® code is reported?
Provider performs staged procedures for gender reassignment surgery converting female anatomy to male anatomy.
What CPT® code is reported?
(What CPT® coding is reported for the insertion ofHeyman capsulesfor clinical brachytherapy?)
When a provider ' s documentation refers to use, abuse, and dependence of the same substance (e.g. alcohol), which statement is correct?
(Full Case:Procedure:Excision of6.0 cm malignant lesionof theright forearmwithadjacent tissue transferusing arotation flap.Pre/Post-op Dx:Basal cell carcinoma, right forearm.Anesthesia:local (1% Xylocaine with epi).Defect size:8 sq cm.Specimen:sent forfrozen section margin control; margins confirmed clear.Closure:rotation flap from adjacent healthy tissue,total area 8 sq cm, secured with layered closure (5-0 Vicryl/6-0 Prolene).Question:What CPT® coding is reported?)
A patient with jaundice was seen by the physician to obtain liver biopsies. A needle biopsy was taken using CT guidance for needle placement. The physician obtained two core biopsies, which
were then sent to pathology. What CPT® codes are reported?
A 13-year-old established patient is seen for an annual preventive exam. Last visit was two years ago.
What CPT® code is reported?
(What doesNCCIstand for, and what is its purpose?)
(A 50-year-old patient undergoesflexible bronchoscopy with bronchial biopsies. Five biopsies are taken and sent to the lab. What CPT® coding is reported?)
A 4-year-old, critically ill child is admitted to the PICU from the ED with respiratory failure due to an exacerbation of asthma not manageable in the ER. The PICU provider takes over the care of the patient and starts continuous bronchodilator therapy and pharmacologic support with cardiovascular monitoring and possible mechanical ventilation support.
What is the E/M code for this encounter?
The provider performs a radical resection of a 4.5 cm sarcoma in the upper arm.
What CPT® coding is reported?
(Day 1: Provider admits patient toobservation carefor type 2 diabetes with hyperglycemia, orders labs, consults endocrinologist, starts IV insulin drip, keeps overnight. Day 2: orders glucose test, dietitian, documents total time 25 minutes. Day 3: glucose normal, documents 15 minutes, discharges patient. What E/M coding is reported by the physician for the patient in observation care?)
(A patient with abnormal growth had asuppression studythat includedfive glucose testsandfive human growth hormone tests. What CPT® coding is reported?)
A physician prescribes carbamazepine to treat a patient with epileptic seizures. After six months, the physician performs a therapeutic drug test to monitor the total level of the drug in the patient.
What CPT® and ICD-10-CM coding is used for the six month-evaluation?
The gynecologist performs a colposcopy of the cervix including biopsy and endocervical curettage.
What CPT® code is reported?
A 35-year-old female has cancer in her left breast. The surgeon performs a mastectomy, removing the breast tissue, skin, pectoral muscles, and surrounding tissue, including the axillary and internal mammary lymph nodes.
Which mastectomy code is reported?
(A 42-year-old female is in the operative room to repair azone 2 flexor digitorum profundus (FDP) tendonlaceration involving her index finger with an associatedradial digital nerveinjury. The dorsal side of the FDP tendon was sutured. Next, themicroscopewas brought into place and the radial digital nerve was repaired using epineural sutures. What CPT® codes are reported?)
(A patient presents to the OR for removal of asubcutaneous cardiac rhythm monitor system14 months after the device was implanted. What is the CPT® code for this service?)
(A dermatologist excises abasal celllesion from an area of thescalp, measuring3.7 cm. This is closed with alayered repair. What CPT® and ICD-10-CM codes are reported?)
A 65-year-old man had a right axillary block by the anesthesiologist. When the arm was totally numb, the arm was prepped and draped, and the surgeon performed tendon repairs of the right first, second, and third fingers. The anesthesiologist monitored the patient throughout the case.
What anesthesia code is reported?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required ? limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What is the radiology coding for this encounter?
(The documentation states: “A punch is placed and pushed downward to obtain a tissue sample for a biopsy of thelunula.” What anatomical structure is being biopsied?)
A patient undergoes lumbar puncture with catheter placement under CT guidance to drain CSF.
What CPT® coding is reported?
(A trauma patient needs the following imaging:2 views nasal bones,3 views chest,2 views left forearm,2 views tibia/fibula. To exclude stroke, aCTA head with contrastis also ordered. What CPT® coding is reported?)
A patient with compression fractures of L5 and the sacrum undergoes vertebroplasty, with cement injected into two vertebral bodies, performed bilaterally.
What CPT® coding is reported?
A 26-year-old male presents with a deep laceration from a kitchen knife to his right hand. The surgeon washes the open wound with sterile saline. Clamps are applied. The provider cleans the
vessel and prepares the edges of thee wound. She then repairs the bleeding vessel with sutures. The clamps are removed and the provider uses a Doppler probe to check the blood flow pattern
through the repaired vessel.
What CPT® code is reported?
A patient with severe diverticulitis in the sigmoid colon presents to surgery for a partial colectomy. The physician performs an exploratory laparoscopic laparotomy to verify the location of the diverticulitis. Once identified, it was noted that there was bleeding from the diverticulitis. The physician transects the descending colon and then transects at the line of the rectum.
The physician mobilizes the splenic flexure in order to create a colostomy with the proximal portion of the remaining colon. The distal portion of the colon is closed. The physician washes the patient ' s abdomen with saline, removes all trocars and instruments, and then closes the abdomen with sutures.
What CPT® and ICD-10-CM codes are reported?
A surgeon performs midface LeFort I reconstruction on a patient’s facial bones to correct a congenital deformity. The reconstruction is performed in two pieces in moving the upper jawbone forward and repositioning the teeth of the maxilla of the mid face.
What CPT® code is reported?
A patient undergoes cystourethroscopy with pyeloscopy and manipulation to remove a ureteral calculus. No stent is inserted.
What CPT® coding is reported?
A patient who has colon adenocarcinoma undergoes an open partial colectomy. The surgeon removes the proximal colon and terminal ileum and reconnects the cut ends of the distal ileum and
remaining colon.
What procedure and diagnosis codes are reported?
A flexible sigmoidoscopy is performed with ablation of two sigmoid colon polyps.
What CPT® and ICD-10-CM codes are reported?
(A 1-year-old patient was born with twosupernumerary digits, one extending from the right pinky and one extending from the left pinky. The digit from his left pinky is larger and includes themetacarpal bone with a jointand is amputated. The one on the right is anubbinand containsno bony structure. The hand surgeon removes the extra digit containingsoft tissueby a simple excision. What is the CPT® coding for the procedures performed?)
Refer to the supplemental information when answering this question:
View MR 005271
What CPT® coding is reported?
A patient comes in complaining of pain in the lower left back, which is accompanied by a numbing sensation that extends into the leg. Attempts to alleviate the pain with home treatments have been unsuccessful. The provider orders an MRI of the lumbar spine initially without, and then with, contrast material. The images are interpreted by the physician, the final diagnosis is left-sided low back pain with sciatica.
What CPT® and ICD-10-CM codes are reported?
(Full Case:Patient:V. Bowen.Physician:C.S., MD.Reason for admission:Abdominal pain.HPI:admitted this morning; sudden onset RUQ pain began ~4:00 p.m. yesterday; started while eating; 8/10; chills/sweating/nausea; no vomiting/diarrhea; last BM 2:00 p.m. yesterday; unable to pass stool or gas since; abdominal distention; poor sleep; prior similar episodes relieved by gas tablets but not this time; no discolored stool/urine.PMH:HTN (losartan; missed dose).PSH:bunion surgery right foot.FH:HTN.SH:no smoking/alcohol.Meds:losartan daily.Allergies:NKDA.ROS:nausea, no emesis; no flatus/stool since yesterday; no weight change; no SOB/chest pain; no jaundice; no urinary frequency/urgency.PE:alert/oriented x3; obvious abdominal discomfort. Vitals 139/100, pulse 100, RR 16, temp 36.4. HEENT normal; CV regular; lungs clear. Abdomen: +BS, soft but very tender; worst RUQ;Murphy’s sign; guarding and rebound (worse with palpation). Extremities trace edema.Labs ordered/reviewed:CMP with abnormal LFT/bili; CBC WBC 9.9; etc.Final assessment:RUQ abdominal pain,rule out cholecystitis.Plan:NPO; morphine IV (controlled substance); IV NS 150 cc/hr; abdominal ultrasound and HIDA ordered; consider surgical consult based on results.Question:What CPT® and ICD-10-CM codes are reported?)
What modifier is appended to indicate when a procedure performed during the postoperative period is unrelated to the original surgery?
A 7-year-old boy is brought to the pediatric clinic by his mother. She reported that her son is complaining of discomfort in both ears and loss of hearing in the left ear for the past two days. The pediatrician diagnosis is impacted cerumen. Pediatrician with the mother ' s consent removes impacted cerumen using water irrigation In the right ear. For the left ear the cerumen impaction is removed using instrumentation.
What CPT® coding is reported '
Which place of service code is submitted on the claim for a service that is performed in a skilled nursing facility?
(A 60-year-old man presents for examination of the entire rectum andsigmoid colon. Two polyps are found in the sigmoid colon and removed usingablation. What CPT® and ICD-10-CM codes are reported?)
The pulmonologist performs a bronchoscopy with fluoroscopic guidance. The scope is introduced into the right nostril and advanced to the vocal cords and into the trachea. The scope is advanced to the right upper lobe and a lung nodule is noted. An endobronchial biopsy is performed.
What CPT® code is reported for the procedure?
A patient underwent a colonoscopy, where the gastroenterologist biopsied two polyps from the colon. Each polyp was sent to pathology as separately identified specimens. The gastroenterologist was requesting a pathology consult while the patient was still on the table. Tissue blocks and frozen sections were then prepared and examined as follows:
Specimen 1: First Tissue Block—Three Frozen Sections Second Tissue Block—One Frozen Section Specimen 2: First Tissue Block—Two Frozen Sections Second Tissue Block—One Frozen Section
What CPT® coding is reported?
(A patient presents with fatigue and unexplained weight gain. To evaluate possible thyroid dysfunction, the provider orders a single laboratory test to measurethyroid-stimulating hormone (TSH). A routine venous blood sample is collected and sent to the laboratory.Which CPT® and ICD-10-CM® codes are reported?)
(The patient presents to the emergency department with chest pain. EKG showsNSTEMIand troponin is abnormal. The ED provider discusses the case with a cardiologist and the patient is admitted for heart catheterization/PCI. What is the E/M service and ICD-10-CM coding reported for the ED provider?)
A patient is diagnosed with a pressure ulcer on her right heel that is currently being treated.
What ICD-10-CM code is reported?
A male patient passes out while jogging in the park. Upon examination at the hospital, he is found to have a wide complex tachycardia and undergoes an electrophysiologic study and radiofrequency ablation. For this procedure he is placed under general anesthesia.
What is the anesthesia coding for this otherwise healthy 35-year-old?
The provider orders a bile test for a patient that has chronic hepatitis that is undergoing treatment. Lab analyst quantitates the total bile acids with an enzymatic method. What CPT® code is
reported for the test?
A 64-year-old with congestive heart failure (CHF) has pericardial effusion. The provider inserts a needle under ultrasound guidance, aspirating the fluid from the pericardial sac.
What CPT® coding is reported?
The patient came in with an inflamed seborrheic keratosis on her nose for a shave removal. After applying local anesthesia, a 0.7 cm dermal lesion was removed using an 11 blade.
What CPT® and ICD-10-CM codes are reported?
A patient with malignant lymphoma is administered the antineoplastic drug Rituximab 800 mg and then 100 mg of Benadryl.
Which HCPCS Level II codes are reported for both drugs administered intravenously?
A planned partial meniscectomy of the temporomandibular joint is cancelled after anesthesia and incision due to respiratory distress.
What CPT® coding is reported for the oral surgeon?
A patient comes to the gynecologist ' s office to check if she is pregnant. A urine sample is taken and tested. The visual result is positive that she is pregnant.
What CPT® code is reported '
Multiple laceration repairs were performed:
Simple: cheek (2.5 cm), nose (3 cm)
Intermediate: left leg (9 cm), right leg (11.5 cm)
Complex: left upper arm (4 cm)
What CPT® codes are reported?
The patient, who is at 32 weeks pregnant, has been hospitalized due to an infection of COVID-19.
What ICD-10-CM codes are reported?
A therapeutic colonoscopy is performed, where the scope goes beyond the splenic flexure, but not to the cecum. Using the Colonoscopy Decision Tree illustrated in the CPT® code book, what coding is reported?
A 49-year-old patient arrives with hearing loss in his left ear. Impedance testing via tympanometry is performed.
What CPT® code is reported?
View MR 002395
MR 002395
Operative Report
Pre-operative Diagnosis: Acute rotator cuff tear
Post-operative Diagnosis: Acute rotator cuff tear, synovitis
Procedures:
1) Rotator cuff repair
2) Biceps Tenodesis
3) Claviculectomy
4) Coracoacromial ligament release
Indication: Rotator cuff injury of a 32-year-old male, sustained while playing soccer.
Findings: Complete tear of the right rotator cuff, synovitis, impingement.
Procedure: The patient was prepared for surgery and placed in left lateral decubitus position. Standard posterior arthroscopy portals were made followed by an anterior-superior portal. Diagnostic arthroscopy was performed. Significant synovitis was carefully debrided. There was a full-thickness upper 3rd subscapularis tear, which was repaired. The lesser tuberosity was debrided back to bleeding healthy bone and a Mitek 4.5 mm helix anchor was placed in the lesser tuberosity. Sutures were passed through the subcapulans in a combination of horizontal mattress and simple interrupted fashion and then tied. There was a partial-thickness tearing of the long head of the biceps. The biceps were released and then anchored in the intertubercular groove with a screw. There was a large anterior acromial spur with subacromial impingement. A CA ligament was released and acromioplasty was performed. Attention was then directed to the
supraspinatus tendon tear. The tear was V-shaped and measured approximately 2.5 cm from anterior to posterior. Two Smith & Nephew PEEK anchors were used for the medial row utilizing Healicoil anchors. Side-to-side stitches were placed. One set of suture tape from each of the medial anchors was then placed through a laterally placed Mitek helix PEEK knotless anchor which was fully inserted after tensioning the tapes. A solid repair was obtained. Next there were severe degenerative changes at the AC joint of approximately 8 to 10 mm. The distal clavicle was resected taking care to preserve the superior AC joint capsule. The shoulder was thoroughly lavaged. The instruments were removed and the incisions were closed in routine fashion. Sterile dressing was applied. The patient was transferred to recovery in stable condition.
What CPT® coding is reported for this case?
(From the left femoral artery, the catheter was advanced into the abdominal aorta, andaortographywas performed to view the location of the left inferior phrenic artery. Next the catheter was advanced into theleft inferior phrenicand into theleft superior suprarenal (adrenal) arteryand angiography was performed. The angiography showed no blockage of the left adrenal artery. What CPT® codes are reported?)
(A 45-year-old patient has a history of chronic otitis media in the left ear. The otolaryngologist performs atympanoplastyand doesnot remove the mastoidto repair the patient’s perforated tympanic membrane.What CPT® and ICD-10-CM codes are reported?)
A three-year-old patient is in the operative suite for stage 2 of treatment for double right outlet syndrome. The patient previously had the pulmonary artery banded and is returning for removal of
the pulmonary band and transposition repair of the great vessels via aortic pulmonary reconstruction.
The surgeon performs a time-out and pre-incision review of respiration and BP then the previous sternal incision site is inspected and lightly painted with povidone. Next, reopens the sternal
cavity and inserts central cannulae in the IVC, SVC and ascending aorta for extra corporeal membrane oxygenation (ECMO) bypass, chemical cardioplegia is initiated, stopping the heart and
ECMO is initiated. A physician assistant monitors vitals and oxygenation until heart function resumes. The surgeon carefully incised and removes the Dacron band encircling the pulmonary
artery, with nominal need for dilation. A section of coronary ostia is removed and sutured to the root of the pulmonary trunk. The pulmonary trunk and aortic root are then transected and
transposed to allow for ideal cardiac circulation. Once structural integrity is visually confirmed, the physician assistant is permitted to administer the cardioplegia reversal solution and the
surgeon removes the central cannulae after heart function safely resumes. The sternotomy is closed and the patient is transported to the NICU.
What CPT® codes are reported for the surgery today?
A patient is having X-ray imaging of his abdomen following a traumatic episode. A decubitus, supine, and erect views are performed on the abdomen.
What CPT® is reported?
An inpatient, suffering from hypertension and chronic kidney disease, is administered continuous venovenous hemofiltration. The on-duty nephrologist performs a series repeated low-level evaluation and management services to monitor the patient ' s status.
What is the CPT® and ICD-10-CM coding '
(A patient is in her dermatologist’s office for treatment of recurring psoriatic plaques on the upper back and neck resistant to topical therapy. The dermatologist performsExcimer laser therapyon the upper back (300 sq cm) and neck (100 sq cm), total surface area400 sq cm. What CPT® codes are reported?)
View MR 005398
MR 005398
Operative Report
Preoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Postoperative Diagnosis: Nonfunctioning right kidney with ureteral stricture.
Procedure: Right nephrectomy with partial ureterectomy.
Findings and Procedure: Under satisfactory general anesthesia, the patient was placed in the right flank position. Right flank and abdomen were prepared and draped out of the sterile field. Skin incision was made between the 11th and 12th ribs laterally. The incision was carried down through the underlying subcutaneous tissues, muscles, and fascia. The right retroperitoneal space was entered. Using blunt and sharp dissection, the right kidney was freed circumferentially. The right artery, vein, and ureter were identified. The ureter was dissected downward where it is completely obstructed in its distal extent. The ureter was clipped and divided distally. The right renal artery was then isolated and divided between 0 silk suture ligatures. The right renal vein was also ligated with suture ligatures and 0 silk ties. The right kidney and ureter were then submitted for pathologic evaluation. The operative field was inspected, and there was no residual bleeding noted, and then it was carefully irrigated with sterile water. Wound closure was then undertaken using 0 Vicryl for the fascial layers, 0 Vicryl for the muscular layers, 2-0 chromic for subcutaneous tissue, and clips for the skin. A Penrose drain was brought out through the dependent aspect of the incision. The patient lost minimal blood and tolerated the procedure well.
What CPT® coding is reported for this case?
(A 5-year-old patient has a fractured radius. The orthopedist providesmoderate sedationand the reduction. The intra-service sedation time is documented as21 minutes. What CPT® code is reported for the moderate sedation?)
A cardiologist attempted to perform a percutaneous transluminal coronary angioplasty of a totally occluded blood vessel. The surgeon stopped the procedure because of an anatomical problem creating risk for the patient and preventing performance of the catheterization.
What modifier is appended to the procedure code?
(A patient presents for an outpatient physical therapy evaluation due to chronic low back pain. The medical record documents that the patient has a current diagnosis oflumbar spine region cancer, which isactively being treatedat the time of therapy. Which lumbar spine associated conditionM codeis reported?)
A patient is diagnosed with sepsis due to enterococcus. What ICD-10-CM code is reported?
A patient with suspected gynecologic malignancy undergoes laparoscopic staging including bilateral pelvic lymphadenectomy, periaortic lymph node sampling, peritoneal washings, peritoneal and diaphragmatic biopsies, and omentectomy.
What CPT® coding is reported?
Patient has cervical spondylosis with myelopathy. The surgeon performed a bilateral posterior laminectomy with facetectomies at each level and foraminotomies performed between interspaces C5-C6 and C6-C7. Bilateral decompression of the nerve roots is achieved.
What CPT® coding is reported?
A patient has chronic cholesteatoma in the right middle ear. The otolaryngologist performed a tympanoplasty with a radical mastoidectomy, removing the middle ear cholesteatoma. Grafting
technique was used to repair the eardrum with ossicular chain reconstruction.
What CPT® code is reported for this surgery?
(A provider orders a liquid chromatography mass spectrometry (LC-MS) definitive drug test for a patient suspected ofacetaminophen (analgesic) overdose. What CPT® code is reported for the test?)
3 Months Free Update
3 Months Free Update
3 Months Free Update

TESTED 04 Jul 2026