We at Crack4sure are committed to giving students who are preparing for the NCC EFM Exam the most current and reliable questions . To help people study, we've made some of our Certified - Electronic Fetal Monitoring exam materials available for free to everyone. You can take the Free EFM Practice Test as many times as you want. The answers to the practice questions are given, and each answer is explained.
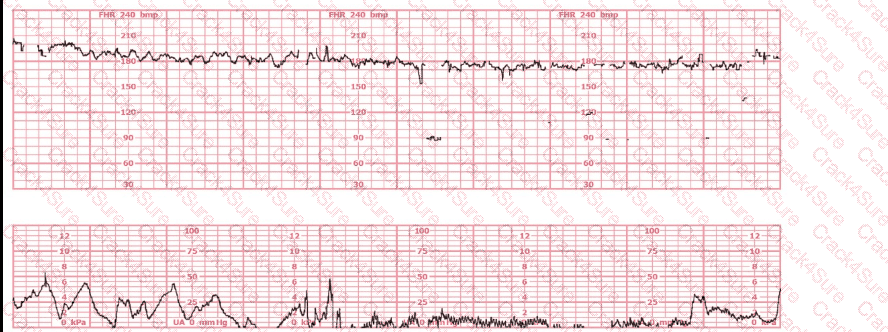
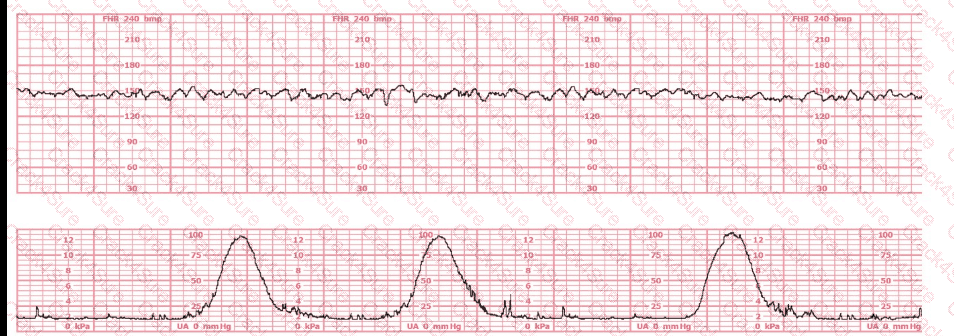
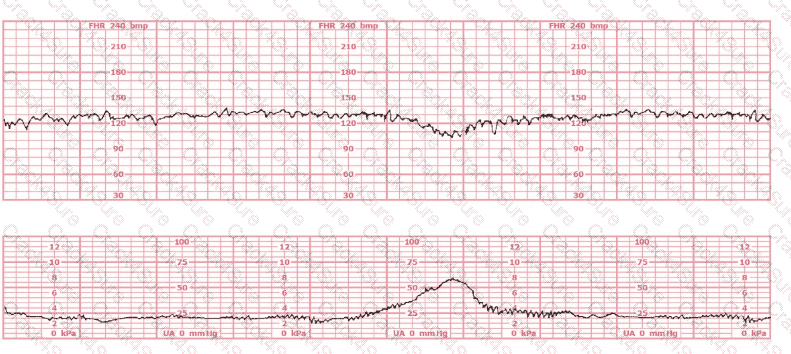
A 30-year-old woman (G2P0) is experiencing preterm labor at 26-weeks gestation. She is receiving magnesium sulfate for neuroprotection. Her external fetal monitoring tracing over the past 30 minutes is shown. The next step would be to:
When R-R intervals are short, the fetal heart rate is
The tracing shown is a:
A 30-minute tracing with moderate variability, accelerations, and one variable deceleration would be classified as:
Maternal conditions of autoimmunity can result in fetal heart block due to antibodies that target:
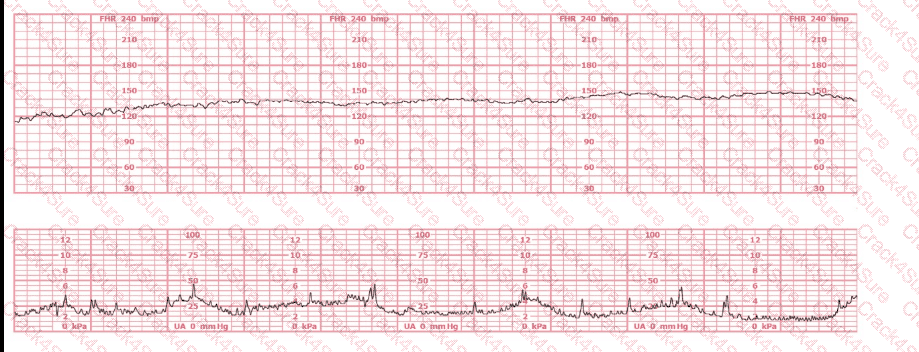
This is a tracing of a multiparous woman in the second stage of labor. The vertex is at +3 station. This pattern has continued for the last 20 minutes. She has been pushing for 2½ hours, and oxytocin is infusing at 12 milliunits/minute. Management should include
When accelerations precede a variable deceleration pattern, this is caused by
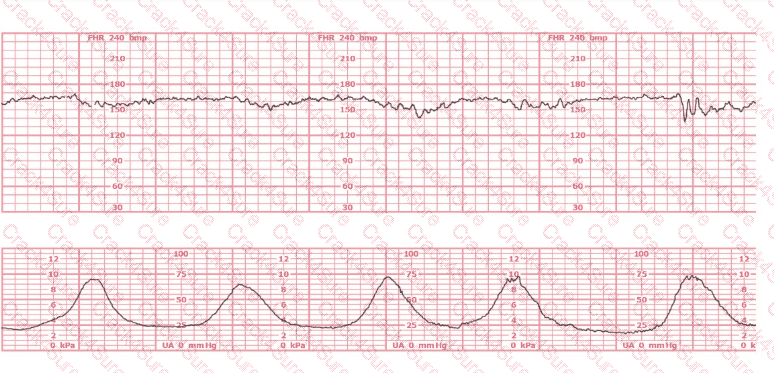
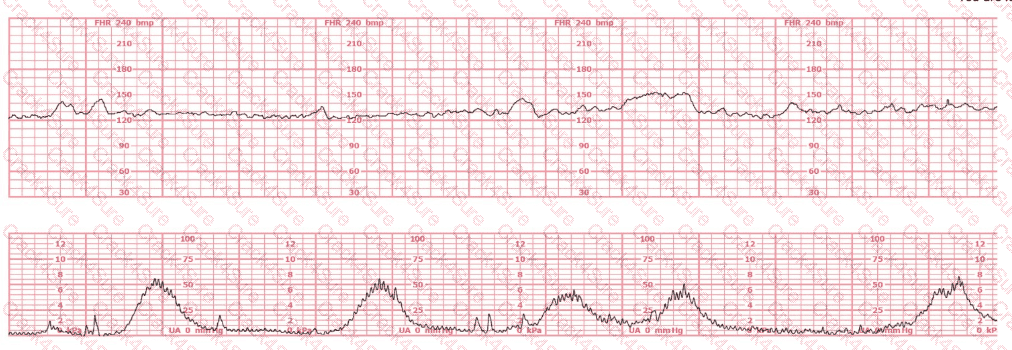
A woman (G1, P0) at 41-weeks gestation presents to OB triage to rule out labor. Her cervical exam is 1 cm/50%/-2. Membranes are intact. She would like to go home if not in labor. Based on this tracing, which represents the last two hours, the best approach is:
This tracing reflects
In the event of recurrent variable decelerations with thick meconium, amnioinfusion is recommended to:
(Full question statement)
A dysrhythmia is noted. The pregnancy and labor course has been normal with no complications. The next step in management is to
This fetal heart rate tracing represents:
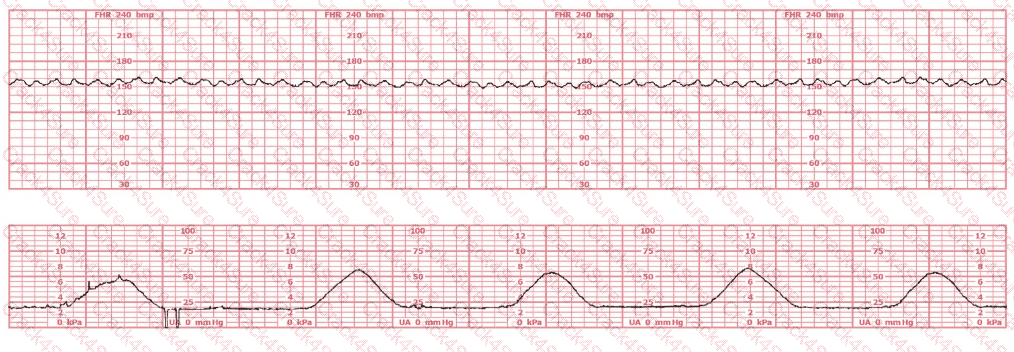
A woman at 38-weeks gestation is admitted to labor and delivery following a fall down the stairs three hours ago. She started feeling contractions in the ambulance. The fetal heart rate tracing shown is on initial evaluation and represents 25 minutes. This tracing is most consistent with a
The most common fetal heart rate pattern consistent with uterine rupture is
This is a fetal heart rate tracing of a multiparous woman whose cervix is 7 cm dilated on admission. The most likely cause for this pattern is:
Patient safety is enhanced when alarms:
A woman in active labor at 8 cm experiences spontaneous rupture of membranes and acute bright red vaginal bleeding. The uterus is soft and nontender to palpation. The fetal monitor tracing has been normal and now shows tachycardia followed by bradycardia with minimal variability. The maternal blood pressure is 130/76 mm Hg, and the pulse is 86 beats per minute. The most likely cause of these findings is:
The pattern on the fetal heart rate tracing shown is likely due to
Interventions to decrease uterine activity should take place:
A woman experiences an eclamptic seizure during the second stage of labor. An anticipated fetal heart rate abnormality post-seizure would be:
Interventions undertaken to address fetal tachycardia are targeted at maximizing
A woman at 36-weeks gestation comes in because of uterine contractions radiating to the back. She has no insurance. In accordance with the Emergency Medical Treatment and Active Labor Act (EMTALA), she is obligated to be:
An internal electronic fetal monitor tracing continues to record artifact despite equipment troubleshooting and replacement of the spiral electrode. The next action is to:
The decelerations seen in the fetal monitoring tracing shown are best described as:
During amnioinfusion, the infusion should be stopped periodically to assess changes in:
A fetus displays a baseline heart rate of 125 beats per minute with moderate variability. During a contraction, the baseline rate drops abruptly to 80 beats per minute with gradual return to baseline over 90 seconds. This is classified as:
(Full question statement)
A woman at 39-weeks gestation is in labor, progressing normally. The baseline fetal heart rate has increased from 125 to 150 beats per minute over the last hour with moderate variability. What is the next step?
The most highly oxygenated blood in the fetal circulation is found in the
Stimulation of the vagus nerve in a healthy fetus will cause:
A pattern of recurrent variable decelerations would move from Category II to Category III if what fetal heart rate change occurs?
When documenting the occurrence of late decelerations in the medical record, what should be charted?
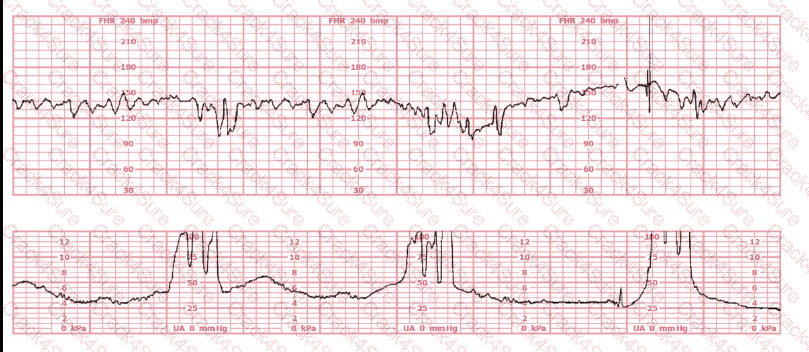
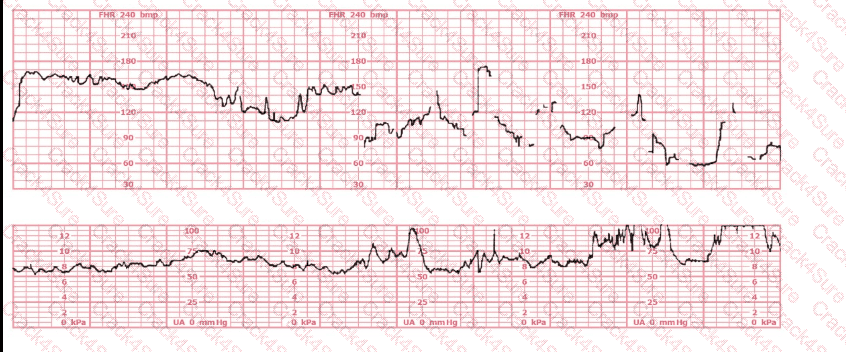
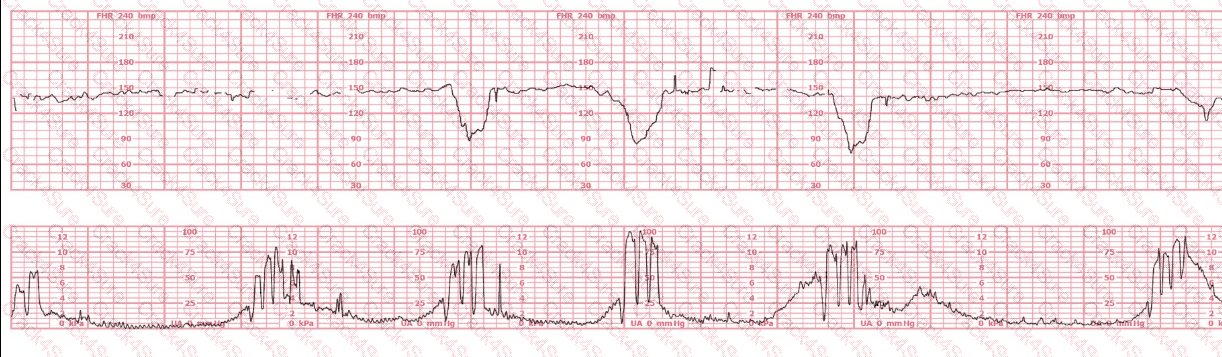
A woman in labor has been pushing for 4 hours. For the last 2 hours, there have been recurrent variable decelerations. Variability has evolved from moderate to minimal. Cervical exam is 10/100%/+2, fetal head OP. There has been no fetal descent for the last 45 minutes. Based on the tracing shown, the most reasonable approach is
3 Months Free Update
3 Months Free Update
3 Months Free Update

TESTED 18 Jul 2026